Tobacco Control
More than a billion people still use tobacco products worldwide due to failure to fully implement proven tobacco control measures.
Curbing the tobacco epidemic is a global health priority to reduce the burden of cancer and other chronic diseases. The World Health Organization Framework Convention on Tobacco Control, the first global public health treaty, entered into force in 2005 and developed a set of six key tobacco-control measures (MPOWER, Map 34.1).
By 2024, it has 183 parties, covering more than 90% of the world population, and has significantly reduced tobacco use among adults from one in three in 2000 to one in five in 2022 (Figure 34.1). Yet more than two billion people worldwide remain without protection from complete MPOWER policies.
The status of selected tobacco control policies in 195 countries, 2022
Footnote
For [M]onitoring, "complete policies" refers to "recent, representative, and periodic data for both adults and adolescents"; blue refers to "recent and representative data for both adults and adolescents; and light blue refers to "recent and periodic data for either adults or adolescents".

“Everyone deserves to live a healthy life free from commercial tobacco-related disease and premature death.”
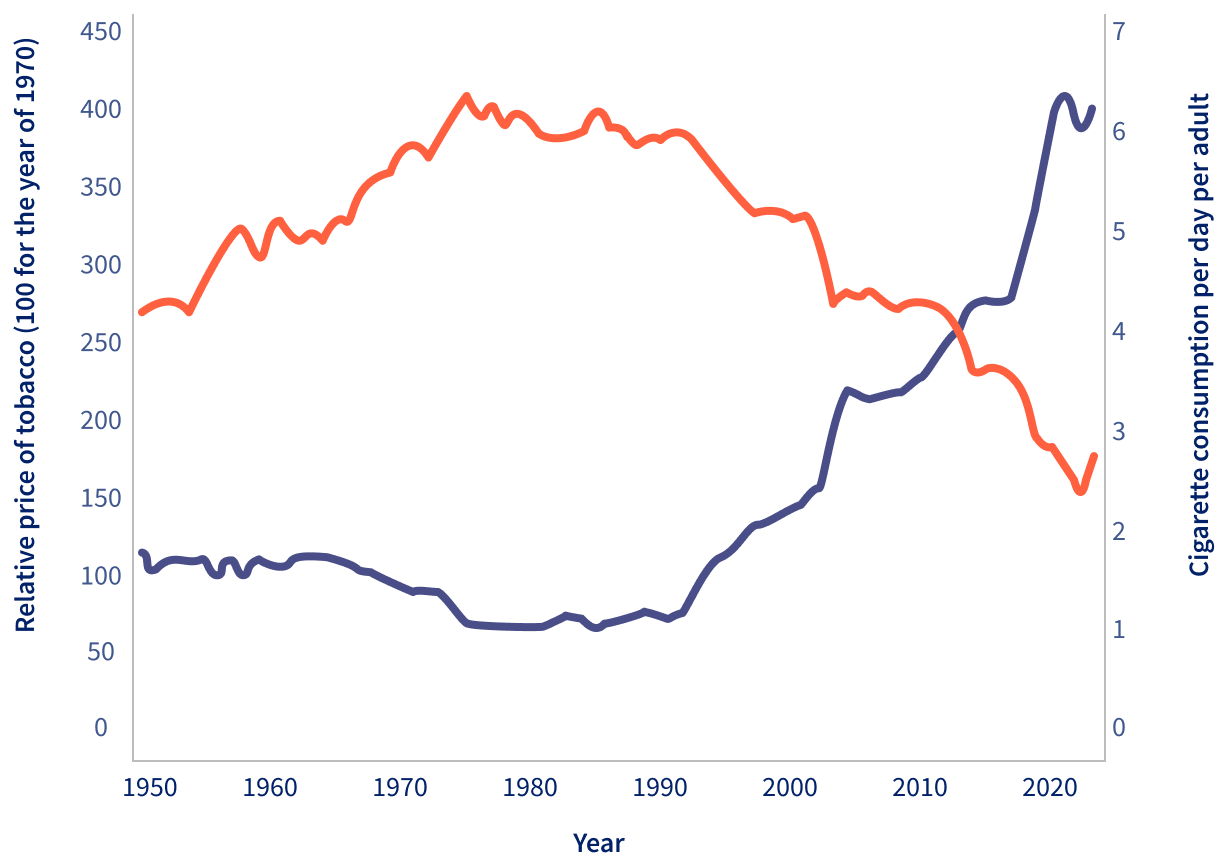
Evidence-based best practices in tobacco-control policies include monitoring tobacco use, treatment for tobacco use, effective warnings about the harms of tobacco use, enacting and enforcing tobacco advertising and sponsorship bans, protecting people from exposure to secondhand smoke and aerosol, and raising tobacco taxes. Raising the tobacco tax has proven to be the most effective and fastest-acting measure of all (Figure 34.2).
Raising prices through taxation is the most effective way to reduce tobacco use.
Tobacco product price and cigarette consumption, France, 1950-2015
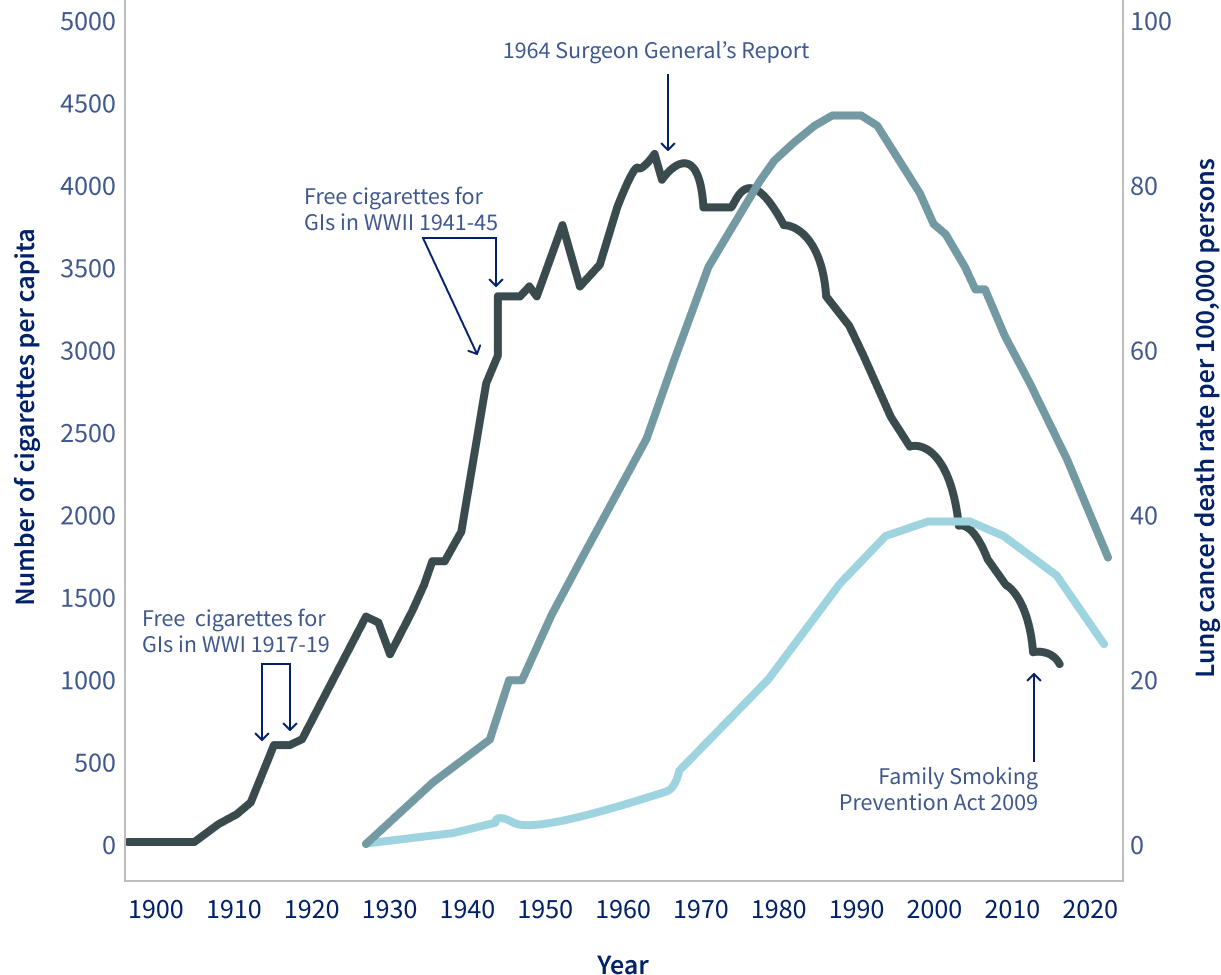
The payoff to investment in tobacco control is high and reflected in improvements in health, productivity, and standards of living (Figure 34.3).
The rise and fall of lung cancer mortality rates closely follow trends in tobacco use, albeit with at least a 25-year lag, reflecting the delayed impact of smoking on public health.
Trends in tobacco consumption and lung cancer mortality rates by sex in the United States, 1900-2020
Footnote
Age adjusted to the 2000 US standard population. Rates exclude deaths in Puerto Rico and other US territories. Note: Due to changes in ICD coding, numerator information for mortality rates has changed over time.
To accelerate progress further, several of these countries are proposing and/or adopting “Endgame Strategies,” which include plain tobacco product packaging, phasing out tobacco sales to younger generations (sales are not allowed to people born after a certain date), reducing nicotine in cigarettes and other combusted tobacco products to non-addictive levels, and reducing the volume and density of tobacco retailers.
Raising the tax on tobacco is not only the most effective tobacco-control policy, but it also raises revenue for other health programs.
Yet, uneven progress in tobacco control policies and implementation has left many low- and middle-income countries behind, where 80% of the world’s 1.3 billion tobacco users live (Map 34.1). Moreover, smokeless tobacco (e.g., chewed tobacco, snuff, snus) has been neglected in tobacco control and continues to cause life-threatening diseases like head and neck cancers. The rise of non-combusted tobacco products (e.g., electronic cigarettes or e-cigarettes, heated tobacco products) and the epidemic of youth e-cigarette use in many countries present further challenges (Figure 34.4). Despite substantial progress, a long road lies ahead to end the tobacco epidemic through the effective and innovative implementation of tobacco-control policies.